Category: Bipolar Disorder

 By Danielle Johnson, MD, FAPA
By Danielle Johnson, MD, FAPA
Chief Medical Officer, Lindner Center of Hope
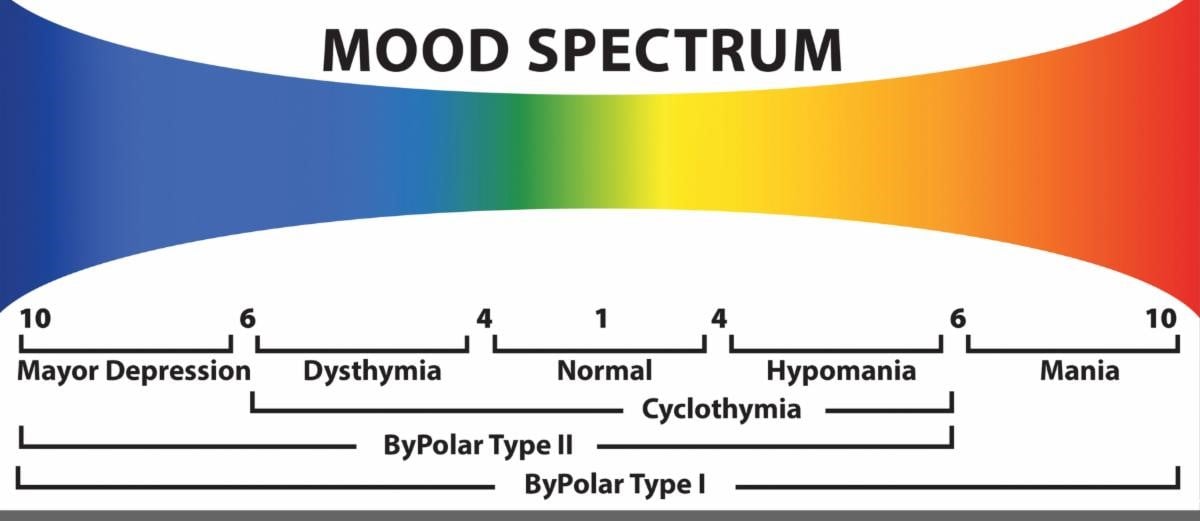
Mood disorders have distinct disturbances in emotions. Low moods are called depression and high moods are called hypomania or mania. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) categorizes mood disorders into bipolar disorders and depressive disorders. Mood disorders include major depressive disorder, bipolar I and bipolar II disorder, disruptive mood dysregulation disorder, premenstrual dysphoric disorder, persistent depressive disorder, and cyclothymic disorder. In the U.S., almost 1 in 10 (9.7%) adults experienced any mood disorder in the past year, with past year prevalence of any mood disorder being higher for females (11.6%) than for males (7.7%). More than 1 in 5 (21.4%) U.S. adults will experience any mood disorder in their lifetime. Mood disorders are common in children and adolescents with an estimated 15% having any mood disorder. Major depressive disorder and bipolar disorder are the most common mood disorders with 8.3% of all U.S. adults experiencing at least one major depressive episode in the past year and 2.8% of U.S. adults having bipolar disorder in the past year.
When people experience symptoms of a mood disorder that do not look like major depression or bipolar disorder this can lead to a delay in diagnosis and treatment as they might have difficulty articulating their symptoms and healthcare professionals might not ask questions about other disorders. Although other mood disorders are less common and less severe, they still impact quality of life and functioning.
Persistent depressive disorder (dysthymia) was added to DSM-5 in 2013, combining some criteria of dysthymic disorder and chronic major depressive disorder. With PDD, depressed mood occurs for most of the day, for more days than not, for at least two years (one year for children and adolescents). During a two-year period (one year for children or adolescents), a person has never been without symptoms for more than two months at a time. A major depressive episode can occur before PDD, or people can experience “double depression” when major depressive episodes occur during PDD.
Symptoms can include poor appetite or overeating; insomnia or hypersomnia; low energy or fatigue; low self-esteem; poor concentration or difficulty making decisions; or feelings of hopelessness. PDD is associated with greater childhood adversity and maltreatment, childhood loss of a parent, earlier onset of depression, and higher rates of chronic depression in relatives. People with PDD also experience a higher number of traumatic events during their lifetime. The 12-month prevalence ranges from 0.5% to 1.5%.
Cyclothymic disorder consists of episodes of hypomanic and depressive symptoms that do not meet the full criteria for bipolar or major depressive disorder. The lifetime prevalence is approximately 0.4%-1%. Symptoms last two years, for more days than not with stability of mood for no longer than two consecutive months. Symptoms of depression can include depressed mood, irritability, hopelessness, helplessness, insomnia, fatigue, anhedonia, avolition, negativity of affect, and suicidal ideation. Hypomanic symptoms can include impulsivity, grandiosity, racing thoughts, increased sociability, excess physical activity, and increased speech production.
People with cyclothymia may experience emotional lability, hypersensitivity, recurrent interpersonal altercations, incidents of self-harming, episodes of excessive gambling, reckless sexual activity, multiple divorces, legal or financial problems, and recurrent job loss. The chronic and pervasive nature of cyclothymic disorder can lead to misdiagnosis with cluster B personality disorders.
There are no FDA-approved medications for PDD or cyclothymic disorder. Your psychiatrist or psychiatric nurse practitioner will take a thorough history including past medical history, previous medical trials, and other psychiatric diagnoses and work with you to develop a treatment plan and choose appropriate medications and psychotherapy to treat depressive and/or hypomanic symptoms.
Sekhon S, Gupta V. Mood Disorder. [Updated 2023 May 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK558911/
https://www.nimh.nih.gov/health/statistics/any-mood-disorder
https://www.nimh.nih.gov/health/statistics/major-depression
https://www.nimh.nih.gov/health/statistics/bipolar-disorder
Patel RK, Aslam SP, Rose GM. Persistent Depressive Disorder. [Updated 2024 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK541052/
Patel RK, Aslam SP, Rose GM. Persistent Depressive Disorder. [Updated 2024 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: